

Биспектральный индекс (BIS) – это недавно обработанный параметр электроэнцефалограммы, который был специально разработан для измерения снотворных эффектов анестезии. Исследования показали, что мониторинг BIS позволяет лучше титровать анестезию, что приводит к снижению потребления снотворных препаратов и улучшению выздоровления. Титрование анестетиков с помощью BIS обеспечивает клинические и экономические преимущества, оправдывающие его рутинное использование. Существуют и другие мониторы «глубины анестезии» (например, энтропия). В этой статье дается краткое описание клинического использования мониторинга BIS и того, как он может улучшить результаты анестезии.
The Bispectral Index (BIS) is a newly processed electroencephalogram parameter that was specifically developed to measure the hypnotic effects of anesthesia. Studies have shown that BIS monitoring allows better titration of anesthesia, resulting in lower hypnotic drug use and improved recovery. Anesthetic titration with BIS provides clinical and economic benefits to justify its routine use. Other «depth of anesthesia» monitors exist (e.g. Entropy). This article summarizes the clinical use of BIS monitoring and how it can improve anesthetic outcomes.
The BIS was introduced by Aspect Medical Systems, Inc. in 1994 as a novel measure of the level of consciousness by algorithmic analysis of a patient’s electroencephalogram during general anesthesia [1]. It is used to measure the depth of sedation or anesthesia. BIS monitoring systems are intended to be used by trained healthcare personnel on adult and pediatric patients to monitor the state of the brain by data acquisition of EEG signals. It is important that the level of general anesthesia (GA) is appropriate for the individual patient undergoing surgery. If anesthesia is deeper than required to keep a patient unconscious, there might be increased risk of anesthetic-related morbidity, such as postoperative nausea, vomiting and cognitive dysfunction. This may also prolong recovery times, potentially increasing health-care costs. If anesthesia is too light, patients may not be fully unconscious and could be at risk of intraoperative awareness [2].
Bispectral Index (BIS) Monitoring
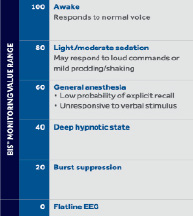
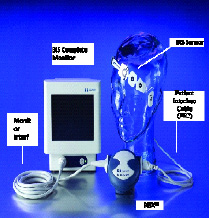
The BIS device consists of a transducer that is connected to a monitor on one end and the patient’s forehead via an adhesive electrode sensor strip on the other. The two to four sensors on the strip each have numbers that indicate where on the forehead they should be placed for optimal EEG signal analysis. The monitor calculates the data received by the two to four sensors and displays this information as a numeric value from 0 to 100. Each numerical range correlates to a degree of sedation which correlates with important clinical endpoints and EEG states during administration of anesthetic agents. 100 represent an «awake» while 0 denotes the maximal suppressed EEG effects [3].:
BIS is a complex monitoring technology intended for use as an adjunct to clinical judgment and training. Clinical judgment should always be used when interpreting the BIS in conjunction with other available clinical signs. Reliance on the BIS alone for intraoperative anesthetic management is not recommended. Certain anesthetic medications do not perform as expected with BIS monitoring e.g. nitrous oxide or ketamine can increase or not change the BIS value. This may be because the BIS values are known to correlate well with the cerebral metabolic rate (CMR) and both drugs, in contrast to other anesthetic agents, are known to increase CMR [3].
BIS Index values may reflect the reduced cerebral metabolic rate produced by most hypnotics. A significant correlation between BIS™ monitoring values and reduction in whole brain metabolic activity due to increasing anesthetic effect was measured using positron emission tomography (PET) scan [4].
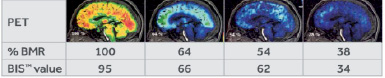
Significant correlation is seen in the figure above between decreasing brain metabolic rate ( % BMR = percent of initial whole-brain glucose metabolism measured from PET scan) and increasing anesthetic effect (as measured by decreasing BIS™ monitoring value). BIS™ monitoring value provides a measurement of brain state derived from the EEG changes in response to changes in the brain. BIS™ monitoring values decrease during natural sleep as well as during administration of a sedative or an anesthetic agent [4].
Entropy and Bispectral Index Monitoring in Anesthesiology
Both entropy and the bispectral index are claimed to be good measures of the hypnotic component of anesthesia but there may be differences between calculated index values. State entropy is based on the spectral entropy, which is obtained by the application of Shannon entropy to the power spectrum. It characterizes the frequency distribution calculated from frontal EEG (0.8 to 32 Hz). To measure the depth of anesthesia, EEG signals are analyzed during anesthesia. Among the EEG-derived indices, the bispectral index (BIS™, Aspect Medical Systems, Newton, MA) is widely used and documented in estimating the hypnotic level during general anesthesia. This index has proven to be a highly sensitive and specific measure of the anesthetic effect in comparison with other EEG-derived variables. Anaesthetic depth can also be measured by means of spectral entropy with the use of tools such as the Datex-Ohmeda S/5 Entropy™ Module (Datex-Ohmeda Division, Instrumentarium Corp., Helsinki, Finland) [5]. It is now possible to acquire and process raw EEG and frontal EMG (fEMG) signals to produce two spectral-entropy-based indices (response entropy and state entropy) reflective of nociceptive and hypnotic levels during general anesthesia. State Entropy (SE, range 0–91) and Response Entropy (RE, range 0–100). Low Entropy numbers indicate unconsciousness. SE uses the frequency range 0.8–32 Hz, representing predominantly the EEG activity whereas; RE is calculated at 0.8–47 Hz, consists of both EEG and facial EMG.

The integration of BIS monitoring with other traditional monitoring has created new paradigms for intraoperative patient assessment and management. BIS value used in combination with hemodynamic data and patient assessment can facilitate the rational selection of sedatives, analgesics and autonomic blockers.
Example: Each anesthetic drug has its own EEG signature that reflects its site of action [6]:
– Propofol acts at the GABA receptor and has this signature:

– Ketamine acts at the NMDA receptor:

– Dexmedetomidine acts at the locus coeruleus:

Conclusion
BIS™ technology measures electrical activity in the brain, it provides a direct correlation with level of consciousness (hypnosis). It is not recommended to solely depend on the BIS monitoring for intraoperative anesthetic management. Clinical judgment is crucial when interpreting BIS data. There is no single anesthetic technique that is appropriate for every patient for every clinical situation. Optimum use of BIS monitoring to guide anesthesia care depend upon the clinical goals of the anesthesiologist. Patient assessment should include evaluation of BIS data with hemodynamic status as well as observation of other clinical signs. The BIS value is an additional piece of information that can be incorporated with the available information.